HEALTHCARE INEQUALITY IN
AUSTRALIA: AN ANALYSIS OF REGIONAL ACCESS, SOCIOECONOMIC DISPARITIES, AND
PATIENT EXPERIENCE
Student ID:
Name:
Registered
Tutorial Day/Time/Room:
1.
Introduction:
300 words 10% (270 330 words)
The problem of healthcare
equity and accessibility in healthcare continues to be a thorny issue for the
healthcare system of any country in the world, and Australia is no different
due to its geographically dispersed nature. Achieving equity in providing
healthcare services to everybody irrespective of their geographical location
and socioeconomic background is a critical step to ensuring that the general
population has healthier outcomes and the disparities have been minimized.
There are indications that major disparities exist between the urban and rural
or remote communities in healthcare services, quality, and outcomes. A working
Health Policy Analyst in one of the national public health organizations
assumed the role of assessing the healthcare accessibility and equity based on
the data obtained from the Australian Bureau of Statistics (ABS).
The review is aimed at
finding trends in access to healthcare services in the various regions, Major
Cities, Inner Regional areas, outer regional, and Remote Communities. The
report focuses on socioeconomic disparities as Socio-Economic Indexes of Areas (SEIFA)
offers an understanding of the effects of the disadvantage on healthcare
outcomes. Special focus is put on such major healthcare indicators as the
general practitioner (GP) accessibility, specialist care, after-hours medical
care, telehealth adoption, and the quality of the provided care. These
indicators play an important role in determining the efficiency of the
healthcare system for diverse populations.
The analysis takes into
account the issues of Aboriginal and Torres Strait Islander communities, which
are commonly overrepresented in underprivileged localities and have worse
health outcomes. The concept of structures and data visualization created with
Tableau helps understand the results of this report with clarity and a clear
comparative evaluation of the disparities in regions. It is based on their
implications that this report has stated evidence-based policy recommendations
that have led to increased access to healthcare, a decrease in inequalities,
and a more equitable healthcare system in Australia.
Background: 400 words 10% (360 440 words)
Health
Challenges among Aboriginal and Torres Strait Islander Peoples
In Australia, Aboriginal and Torres Strait Islander people have
long-standing health disparities in relation to the non-Indigenous population.
According to Australian data, released by the Australian Bureau of Statistics
(ABS), Indigenous Australians live shorter lives with disproportionately low
life expectancy and high rates of chronic diseases (Eid, 2026). The rates of
preventable hospitalization and mortality are much greater, and this is an
indicator of the shortcomings of the early intervention and access to primary
healthcare services. Mental health problems and psychological distress also
have a higher occurrence rate, and in most cases. These are usually associated
with intergenerational trauma and disadvantage in society (Zhang et al. 2022).
Such inequalities reveal institutional problems in the healthcare delivery
system and underscore the need for interventions.
Socioeconomic
and Environmental Determinants
Social determinants promote or hinder the health outcomes of the
Indigenous populations. It is evident that Aboriginal and Torres Strait
Islander peoples tend to be associated with lower income levels, elevated
unemployment rates, and low levels of attained education (Bammert et al. 2024).
The communities also experience congested or poor housing, clean water, and
sanitation, especially in the remote communities. Indigenous populations are
always found to be in the lowest of the five quintiles in the SEIFA (Atkins
& Mukhida, 2022). These societal economic situations make people
susceptible to diseases, decrease their access to health care systems, and
drive persistent health disparities.
Geographic
Inequality and Healthcare Access
Geographic location is very important in determining healthcare
accessibility. A major percentage of the Indigenous Australians inhabit the
regional and remote regions where there is a lack of healthcare facilities (Walker
et al. 2023). ABS data points out the reduced access to general
practitioners, specialist services, and after-hours in such areas. The effects
of this are delayed diagnoses, greater reported unmet healthcare needs, and
greater use of emergency healthcare (Hassan et al. 2024). Though some regions
have enhanced accessibility to telehealth services, digital barriers and poor
connectivity are still a challenge to the successful implementation of
telehealth services.
Ethical
Frameworks and Indigenous Perspectives
Indigenous health data need to be analysed with ethical frameworks
with the central focus on cultural safety, equity, and respect for the
Indigenous systems of knowledge. Ethical methods mean that information is
viewed most responsibly and does not promote deficit-based discourses (Adams et
al. 2025). To create effective health policies, it is necessary to
incorporate Indigenous and community-led solutions. Culturally appropriate care
and self-determination are frameworks that help address those who do not fit
into the fabric of healthcare planning and lead to the reduction of the
historically existing gap in terms of health outcomes.
Findings: 1000 words 10% (900 1100 words)
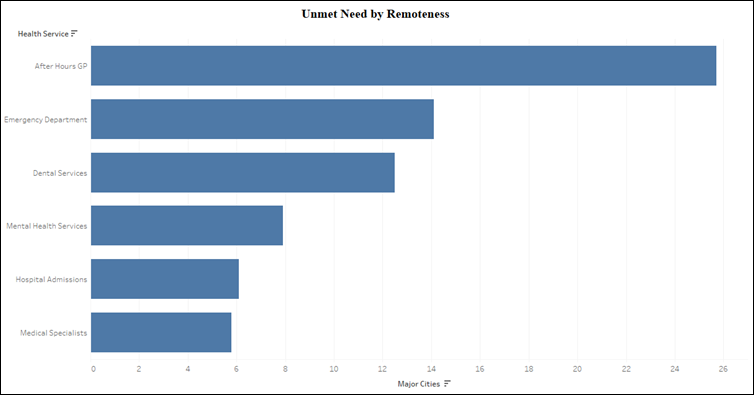
Figure 1: Unmet Need by Remoteness
The figure shows the intensity of unmet healthcare needs of the
various health services among major cities, showing the lack of service access
among people. The chart indicates that the unmet demand in the after-hours GP
service is the highest, which means that patients are unable to seek medical
attention during the non-working hours. Needs that are not met in the emergency
department and dental services also show a high degree of pressure on the
urgent care, and a lack of affordable dental services.
The services, such as hospital admissions and medical specialists,
manifest significantly less unmet demand. It does not always mean that these
are adequately welcomed, since plenty of delays and waiting times are still
seen. The general trend indicates the problems in the healthcare structure that
are present in delivering timely and accessible primary care (Gautam et al. 2024).
These results affirm that even with urbanization, there are still gaps in
healthcare access, and the circumstances must be worse at regional and remote
locations. Only supports the claim that interventions of the policy-making are
aimed at addressing the availability of services and care after working hours.
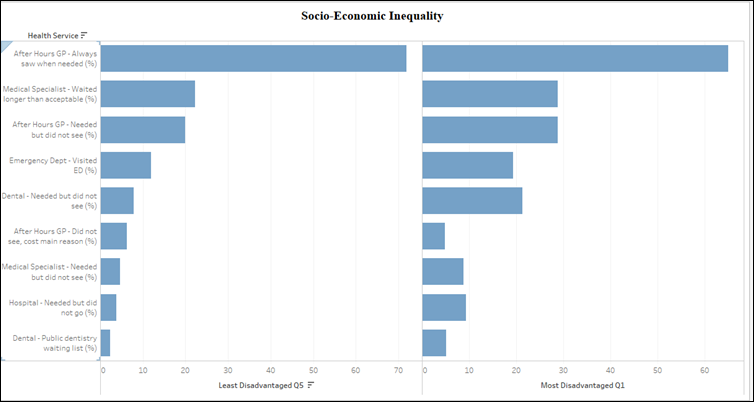
Figure 2: Socio-Economic Inequality
The figure compares healthcare access and outcomes between the least
disadvantaged (Q5) and most disadvantaged (Q1) populations using SEIFA
quintiles. As has been concluded on the chart, people belonging to the group of
the most disadvantaged have much worse healthcare results. As an example, a
greater proportion of individuals in Q1 indicate unsatisfied needs, delays
during consultations with specialists, as well as the inability to receive
after-hours GP consultations when it is needed.
The people in Q5 have better access, as these have greater rates of
obtaining care at the time of need and lower rates of unmet need. The
differences are seen especially in preventive and specialist services, where
the factors of financial and geographic barriers are largely involved. The
socioeconomic status is closely linked to health outcomes, as illustrated by
this inequality (Bertelsen et al. 2025). The findings underscore the
importance of specific healthcare policies that are focused on the underprivileged
population groups, are more affordable, and the services are more accessible to
eliminate systemic disparities in healthcare access.
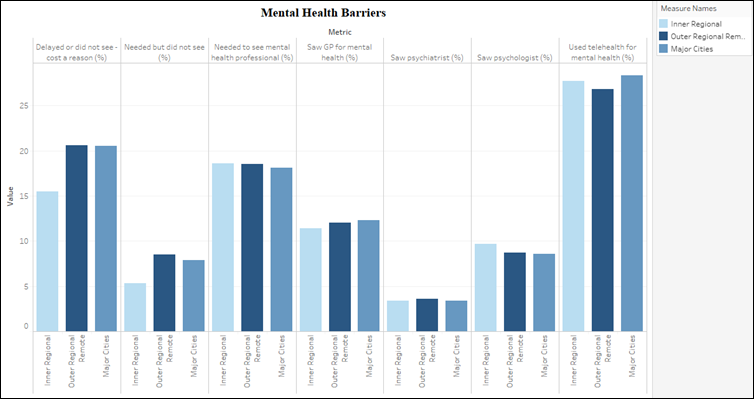
Figure 3: Mental Health Barriers
The figure gives the barriers to access to mental health services in
various areas, comprising major cities, inner regions, outer regions, and
remote areas. The statistics show that people living in the local and remote
territories have more problems with getting mental health care. More
individuals indicate that there is a delay or do not seek healthcare because of
costs, among other factors, which is indicative of financial and access
constraints. Moreover, the number of people in these areas who have access to
mental health services like psychiatrists or psychologists is also low, which
shows that there is a lack of specialized services.
The consultations through GPs are considered particularly more
frequent in mental health, these are not always adequate to address the needs
of a patient, especially in terms of more complicated conditions. There seems
to be some bridging of this gap by telehealth use, particularly in remote
regions; however, it cannot be deemed adequate to eradicate disparities (Yuan et
al. 2025). The number illustrates the important weaknesses in the provision
of mental health care, and it is stressed that a better infrastructure,
workforce allocation, and affordability in underserved areas are required.
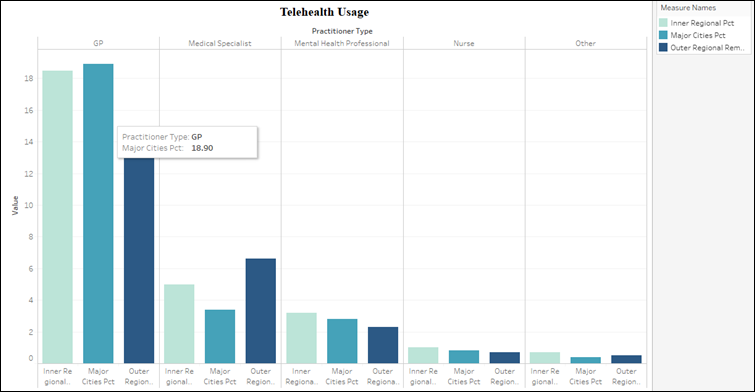
Figure 4: Telehealth Usage
The figure represents the use of telehealth by practitioners of
various types and regions, such as general practitioners, specialists, mental
health professionals, nurses, and other practitioners. It is apparent in the
chart that the use of telehealth is greatest in GP services, which means that
primary care has embraced best practices in transforming to the digital mode of
healthcare delivery. Specialists and mental health professionals have a
relatively low usage, which implies a restriction in providing complicated care
outside the clinic. There are also regional disparities, where the reliance on
telehealth is an indication of comparably higher reliance in outer regional and
remote regions than in the major cities.
This is an upward trend that depicts the compensation for the lack
of physical access to health services in remote areas through telehealth. The
general reduction in the volume of usage in some of the types of practitioners
may indicate that telehealth is capable of replacing face-to-face consultation
to the full extent (Wu et al. 2025). Such results demonstrate the need
to improve the digital healthcare infrastructure and make sure that the
telehealth services are well incorporated into the existing healthcare
practices to enhance accessibility and equity.
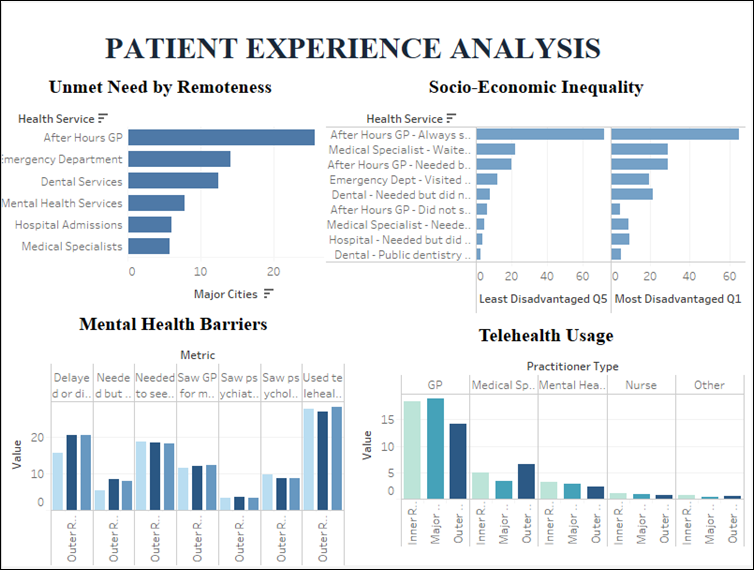
Figure 5: Patient Experience Analysis Dashboard
The figure is a dashboard of several areas of the patient
experience, which include unmet healthcare needs, socioeconomic inequality,
mental health barriers, and telehealth usage. The built-in visualization offers
a comprehensive perspective of the disparities in healthcare within regions and
across groups of people. The dashboard indicates the fact that inequality in
healthcare is a multidimensional problem as it is affected by geographic
location, socioeconomic status, and availability of services. An impoverished
and remote population has even higher needs and mental health barriers, whereas
telehealth has come in as a partial solution to the problem of accessibility.
Comparison among the various charts enables more patterns and
relationships to be identified, which include the relationship between
socioeconomic disadvantage and lack of access to care (Geetha Manukumar et
al. 2026). This dashboard is a strong tool in the decision-making of
policymakers since it provides them with access to complex data. It promotes
policy formulation based on evidence to enhance healthcare equity, better
service delivery, and address systemic disparities in the context of Australia.
Conclusion: 300 words 10% (270 330 words)
The report has critically discussed the accessibility and equity to
healthcare in Australia, specifically pointing out regional inequalities and
the problem of Aboriginal and Torres Strait Islanders. The above picture
clearly describes that it is not possible to have equal opportunities for every
citizen to get well-structured healthcare or treatment. Mostly, it is seen in
the outer regional or rural areas. There is no access to early checkups or
services, nor are there specialists or general physicians. The presence of
socioeconomic disadvantage, which is assessed by SEIFA data, only exacerbates
these disparities, leading to an increased number of unmet healthcare demands
and worse overall health outcomes of the vulnerable groups.
The analysis further establishes that Aboriginal and Torres Strait
Islanders are unfairly burdened by these inequalities since a mix of geographic
remoteness, socioeconomic disadvantage, and structural challenges in the
healthcare system acts to their disadvantage. Although efforts like telehealth
have assisted in enhancing access in remote localities, these are not adequate
to achieve a full-service delivery gap-bridge.
These results support the reason why specific and evidence-based
policy actions are highly required. The national healthcare policies in the
future must be focused on increasing healthcare facilities and healthcare
services in low-income areas, enhancing culturally-sensitive and
community-based healthcare initiatives, and enhancing the practitioner
distribution by offering incentives to medical practitioners in rural
communities. Moreover, digital infrastructure is invested in to ensure optimal
performance of telehealth services.
More importantly,
health inequity is a societal issue that needs a comprehensive approach to the
discussion of social determinants such as education, income, and housing.
Indigenization of the policy-making processes and introducing the indigenous
reasoning and ethical systems contribute to the idea of culturally safe and
inclusive healthcare systems. Further, to ensure the sustainability of changes
to health equity across Australia in the long term, the regular observation of
health data and policy co-design is needed.
References
Adams, C., Walpola, R., Iqbal, M. P., Schembri, A., & Harrison,
R. (2025). The three pillars of patient experience: identifying key drivers of
patient experience to improve quality in healthcare. Journal of Public Health,
33(10), 2105-2113. Retrieve From: https://link.springer.com/article/10.1007/s10389-023-02158-y
[Retrieved On: 1st April. 2026]
Atkins, N., & Mukhida, K. (2022). The relationship between
patients income and education and their access to pharmacological chronic pain
management: a scoping review. Canadian Journal of Pain, 6(1),
142-170. Retrieve From: https://www.tandfonline.com/doi/pdf/10.1080/24740527.2022.2104699
[Retrieve On: 2nd April, 2026]
Bammert, P., Schttig, W., Novelli, A., Iashchenko, I., Spallek, J.,
Blume, M., ... & Sundmacher, L. (2024). The role of mesolevel
characteristics of the health care system and socioeconomic factors on health
care useresults of a scoping review. International Journal for Equity in
Health, 23(1), 37. Retrieve From:
https://link.springer.com/content/pdf/10.1186/s12939-024-02122-6.pdf [Retrieve On: 2nd
April, 2026]
Bertelsen, N., Oehrlein, E., Lewis, B., Westrich-Robertson, T.,
Elliott, J., Willgoss, T., ... & Brooke, N. (2025). Patient engagement and
patient experience data in regulatory review and health technology assessment:
where are we today? Therapeutic innovation & regulatory science, 59(4),
737-752. Retrieve From: https://link.springer.com/article/10.1007/s43441-025-00770-6
[Retrieved On: 1st April. 2026]
Eid, N. M. (2026). Digital health adoption in nutrition care: A
national cross-sectional, Arabic-validated survey and cluster analysis of
patient experience and willingness to use telenutrition in Saudi Arabia.
Digital Health, 12, 20552076261419237. Retrieve From: https://journals.sagepub.com/doi/abs/10.1177/20552076261419237
[Retrieved On: 1st April. 2026]
Gautam, N., Rahman, M. M., Hashmi, R., Lim, A., & Khanam, R.
(2024). Socioeconomic inequalities in child and adolescent mental health in
Australia: the role of parenting style and parents relationships. Child and
Adolescent Psychiatry and Mental Health, 18(1), 28. Retrieve From: https://link.springer.com/content/pdf/10.1186/s13034-024-00719-x.pdf
[Retrieve On: 2nd April, 2026]
Geetha Manukumar, A., Rahimipour Anaraki, N., Etchegary, H., Walsh,
A., Hurley, O., Patey, C., ... & Asghari, S. (2026). Voices from the
emergency department: A theoretical framework analysis on patient experiences
of care in emergency departments of Newfoundland and Labrador, Canada. PLoS
One, 21(2), e0342555. Retrieve From: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0342555
[Retrieved On: 1st April. 2026]
Hassan, M. M., Ameeq, M., Tahir, M. H., Naz, S., Fatima, L., &
Kargbo, A. (2024). Investigating socioeconomic disparities of Kangaroo mother
care on preterm infant health outcomes. Journal of Psychosomatic Obstetrics
& Gynecology, 45(1), 2299982. Retrieve
From: https://www.tandfonline.com/doi/pdf/10.1080/0167482X.2023.2299982
[Retrieve On: 2nd April, 2026]
Walker, A. F., Graham, S., Maple-Brown, L., Egede, L. E., Campbell,
J. A., Walker, R. J., ... & Agarwal, S. (2023). Interventions to address
global inequity in diabetes: international progress. The Lancet, 402(10397),
250-264. Retrieve From: https://www.sciencedirect.com/science/article/am/pii/S0140673623009145
[Retrieve On: 2nd April, 2026]
Wu, K., Dang Nguyen, M., Rouleau, G., Azavedo, R., Srinivasan, D.,
& Desveaux, L. (2025). Understanding how virtual care has shifted primary
care interactions and patient experience: A qualitative analysis. Journal of
Telemedicine and Telecare, 31(1), 73-81. Retrieve From: https://journals.sagepub.com/doi/abs/10.1177/1357633X231167905
[Retrieved On: 1st April. 2026]
Yuan, J., Chen, X., Yang, C., Chen, J., Han, P., Zhang, Y., &
Zhang, Y. (2025). Identifying Patients Preference During Their Hospital
Experience. A Sentiment and Topic Analysis of Patient-Experience Comments via
Natural Language Techniques. Patient preference and adherence, 2027-2037.
Retrieve From: https://www.tandfonline.com/doi/abs/10.2147/PPA.S526623
[Retrieved On: 1st April. 2026]
Zhang, H., Fu, Y., Chen, M., & Si, L. (2022). Socioeconomic
inequality in health care use among cancer patients in China: Evidence from the
China Health and Retirement Longitudinal Study. Frontiers in Public Health,
10, 942911. Retrieve From: https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2022.942911/pdf
[Retrieve On: 2nd April, 2026]
Appendix
Dataset
Link: https://www.abs.gov.au/statistics/health/health-services/patient-experiences/2024-25#data-downloads
 +1 213 5100402
+1 213 5100402
 +61 489 995404
+61 489 995404
 +44 203 7692978
+44 203 7692978
 4.6
4.6
 4.72
4.72
 4.92
4.92